The Prevalence of Neck Pain
In 2017, the Brazilian Journal of Physical Therapy (BJPT) published a study on neck pain that sought to explore the prevalence of neck pain as well as its sociological factors(1).
The result of the 600 person survey was that neck pain has a high prevalence, but also has a significant correlation to other sociological factors, including certain ergonomics related to sitting and leaning.
A term often used clinically for this type of pain is: insidious. Insidious means it comes on in a gradual and subtle way, but leads to injurious effects. The insidious onset is not usually after a major trauma but is mostly related to the concept of structural repetitive microtrauma.
Repetitive microtrauma means that the daily load of postural and ergonomic deviations can accumulate over time and lead to painful dysfunction, often needing some kind of medical intervention.
Explaining the Functional Spinal Unit
Let’s dive into what causes neck pain, but first, let’s discuss a bit about the mechanics of the spine. Chris Centeno, MD summarizes the seminal work of two researchers, Panjabi and White (2):
…each of the 24 levels of the spine (neck, upper back, and lower back) is more than just single parts, but acts as one machine. That’s called the functional spinal unit (FSU).
The best way to think of the FSU is to think about a car. We think about a car as a fully assembled machine, and a car only functions when fully assembled. If it were reduced to its parts, it would not function like a car at all. Similarly, the FSU is more than just its parts, it works by the sum of its parts functioning together. Let’s take a look at what comprises the FSU.
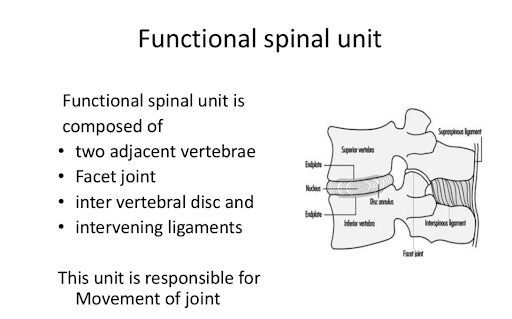
Figure 1 illustrates the basics of one motion segment. It is composed of two vertebrae, the disc between them and the ligaments stabilizing the connecting joints. Then, 24 vertebrae from the upper neck to the lower back are all connected in this way, making the spine a connected string of motion segments, or the Functional Spinal Unit.
To build on the car analogy, one motion segment is analogous to one component of the car’s engine, like a piston, but when all motion segments are functioning together, it’s like the whole car. The interconnected vertebrae allow for the FSU’s interconnected spinal movements in different directions, as seen in Figure 2.
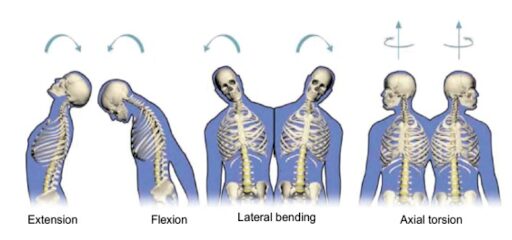
The spine moves as segments within the complete FSU, but if there is dysfunction in one area it serves as a biomechanical chain reaction. And as evidenced above by the study in BJPT, neck pain is commonly associated with postural and ergonomic stressors. Postural stressors in one area has effects on the motion segments above and below and then those affect the segments above and below that, and so on. In short, the FSU is subjected to repetitive mechanical stressors that wreak havoc on the joints, ligaments, and soft tissues of multiple areas.
It’s More Than a Pain Generator
Now that we understand that the FSU is made up of spinal motion segments of vertebrae, discs, joints, and ligaments, we can discuss how different physicians tend to approach pain differently. In traditional orthopedics, physicians target what is called the “pain generator.” This means, if the joints are arthritic, they treat the joints. Or, if there is a disc bulge, they treat the disc. It’s a very mechanistic, monkey see monkey do approach. In regenerative medicine, our physicians look at how the entire FSU can be treated to help address “why” the pain is happening.
What we just learned about the FSU, shows us that there are multiple components at play in each motion segment, which just gets exponentially more involved when we think of multiple vertebrae. Specifically, the cervical spine is made up of seven vertebrae, so that is a large chunk of the FSU, with multiple components involved in even a single motion.
Figure 3 illustrates the interconnectedness of the FSU. Even though this is a low back example, it serves as an analogue to the neck.
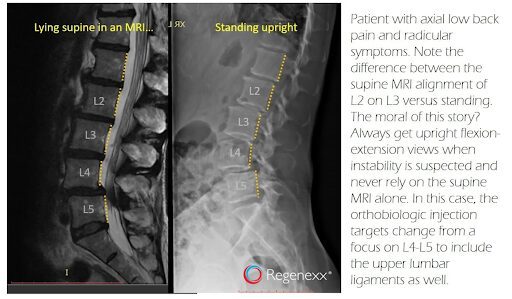
The image on the left is an MRI with the patient laying down and on the right, the patient is standing upright for an X-Ray. This is the same patient. Do you see the difference in how the yellow lines are oriented in the laying versus the standing images? So, let’s say this patient has pain that the physician finds is coming from the L4/L5 area, it would be customary in traditional orthopedics and pain management to treat the joints at L4/5 with cortisone to manage pain, or even some surgeons would fuse that area.
However, if you study the right-hand film, you can see when the patient is upright, they have multiple segments that are sliding forward/backward relative to the motion segments above and below. This is the image of multi-segmental instability. So, fusing or treating one motion segment in the larger FSU will only address a small fraction of the problem. Regenerative Medicine clinicians look at the entire FSU and consider which components are not only pain generators, but structurally contributing to the local and global issues.
Effectively Treating the FSU to Eliminate Pain
The main observation from Figure 3 is that there are multiple levels of spinal instability, despite what the patient’s pain complaint might be. The breadth of this dysfunction outweighs the patient’s physical sensation of pain. Their pain is considered a lagging indicator, meaning that the pain symptoms lagged behind the instability we see. The instability was occurring far before the pain started, so just to treat the pain would miss the boat.
A Regenexx Physician, Chris Williams, MD actually researched the Regenexx registry to seek the trends in patient outcomes as compared to how their spines were treated with Platelet Rich Plasma (PRP)(2). He compared the data from patient-reported outcomes at different time intervals post-procedurally for spine injections. Specifically, he dug into the registry data for patients who had injections just to the facets of the painful joints. Then, he compared those results to patients who had the whole FSU treated with structures including the facet joints, ligaments, and nerves suffering from instability and/or inflammation.
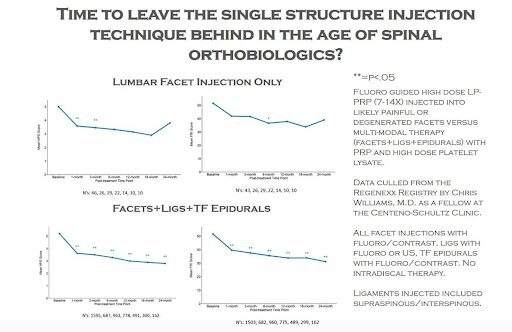
Figure 4 demonstrates the results of this comparison. The lines on all four graphs correlate with a decrease in patient-reported pain. So, we want to see the line go down in these graphs. Notice that using PRP to treat a local facet joint in the top two graphs has a positive effect on the downward trajectory, but then there is an uptick in the line. The lower two graphs show a more decided downward slope from the get-go and do not demonstrate an uptick as time passes. These lower two graphs represent the data from patients who had the entire FSU treated.
What’s the significance of this data review? Well, treating a more comprehensive area with PRP shows that it is increasing stability to the whole FSU. Increasing stability means decreasing those repetitive microtraumas from repetitive postural and ergonomic stressors.
Make sure your physician is looking at your entire body when choosing how to treat your neck pain. A Regenexx physician is not only trained to look at your area of pain, but also at the adjacent areas. As we can see, everything is connected, and treating a broader area can yield more dramatic and longer-lasting results.
References:
- Genebra CV, Maciel NM, Bento TP, Simeão SF, De Vitta A. Prevalence and factors associated with neck pain: a population-based study. Brazilian journal of physical therapy. 2017 Jul 1;21(4):274-80.
- https://regenexx.com/blog/treating-functional-spinal-unit/
- https://www.slideshare.net/sunilsanthosh5/thoraco-lumbar-fractures-of-spine
- https://www.sciencedirect.com/topics/engineering/biomechanical-function
- https://regenexx.com/blog/treating-the-whole-spine-with-orthobiologics/
- https://www.cureus.com/articles/73620-regenerative-injection-treatments-utilizing-platelet-products-and-prolotherapy-for-cervical-spine-pain-a-functional-spinal-unit-approach
- https://ioaregenerative.com/blog/what-is-the-best-treatment-for-cervical-radiculopathy
- https://newregenortho.com/do-it-yourself-exercises-to-help-beat-neck-pain/